


Ready to test your knowledge? Try our ophthalmology questions.
An Approach to Examination of the Eye
A template for examination of the eye for junior doctors, medical students, and membership exams. A systematic approach is useful to ensure a swift and efficient clinical examination.
Introduction
- Wash hands
- Introduce self, confirm patient’s name and date of birth
- A brief history from the patient if not provided
- Explain examination, gain permission, check if patient is happy with privacy
- Check if patient is experiencing any pain or visual disturbance
- Position patient in chair and sit opposite, move around patient as required (e.g. when assessing red reflex)
General Inspection
- Begin with general inspection – is the patient in a hospital bed, with any treatments/monitoring/paraphernalia suggestive of systemic disease?
- Then move to the face – any asymmetry may indicate cranial nerve lesions which can hint that there may be findings on ophthalmic examination
- Comparison with old clinical photographs or a collateral history from a relative may be helpful in determining the degree and timescale of any positive findings on general inspection
Inspection of the eyes
- In a structure like the eye, comparison between sides is crucial in differentiating pathology from normal variation
- Globe
- Proptosis, enophthalmos
- Eyelids/lash margins
- Ptosis, blepharitis, styes, ectropion, entropion, eyelid tumours
- Sclera, conjunctiva, cornea, iris
- Injection, opacities, colour change, discharge
- Pupils
- Please see below
Visual Acuity, Fields, and Colour Vision (CNII)
- To be assessed one eye at a time
- Near vision
- Best assessed using a near-reading chart, can be assessed more crudely with any small print, e.g. newspaper
- Ensure patient wear reading glasses if they use these normally
- Distance vision
- Typically assessed using a Snellen chart – chart 6 metres from the patient, report the lowest line patient can read
- Repeat at a lower distance if unable to read top line, then can assess whether they can see hand movements, or perception of light
- Ensure patient wears glasses if they usually do
- Repeat with a pinhole to assess whether any change in acuity is related to refractive error
- Gross visual acuity can be ascertained by requesting them to look for distant objects such as a wall clock, painting or something far in through the window
- Typically assessed using a Snellen chart – chart 6 metres from the patient, report the lowest line patient can read
- Colour vision
- Assessed using standard Ishihara plates
- Red top of bottles or pen can be used to compare both eyes if color plates not available
- Although traditionally assessed on paper, in busy inpatient settings, electronic versions of all of these tests (e.g. those found on MD Calc) can be useful
Visual Fields
- Assessed clinically using the confrontation test, and quantitively using e.g. Goldmann visual field testing
- Ask patient to cover an eye, mirror them (i.e., if they cover their left eye, cover your right eye)
- Ask them to keep their eye fixed on yours; you do the same
- Assess all four visual quadrants compared to yours by moving a hatpin, pen, or your fingers from outside your visual field, diagonally towards the centre until the patient can see it
- Repeat for the other eye
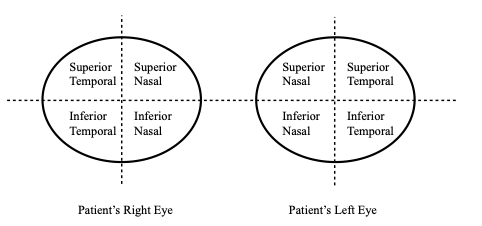
Figure 1. Visual Fields to be Assessed by Confrontation.
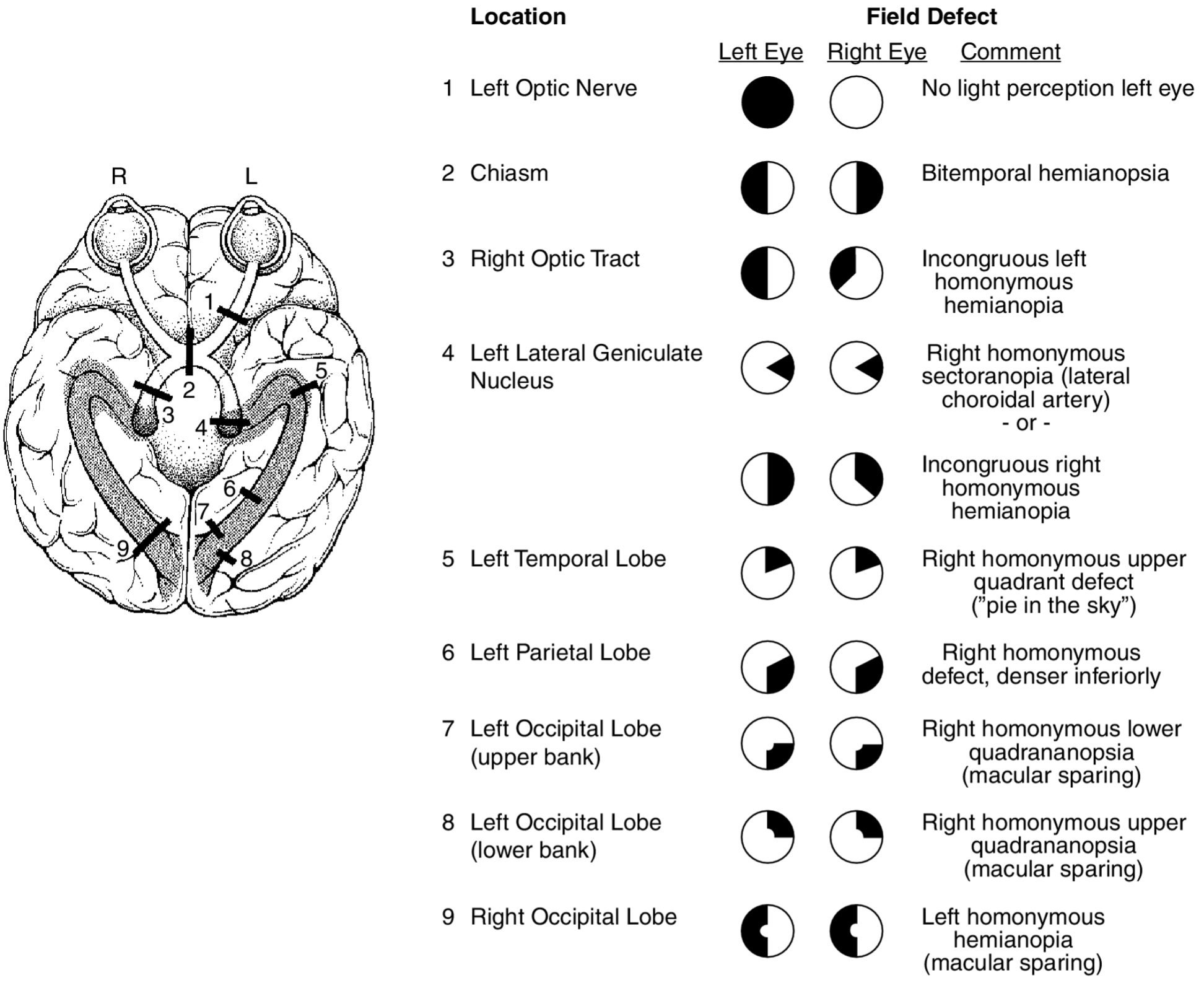
Figure 2. Visual Field Defects and their Corresponding Anatomical Lesions. Credit: Uretsky S. Visual field deficits. In: Ettinger AB, Weisbrot DM, eds. Neurologic Differential Diagnosis: A Case-Based Approach. Cambridge: Cambridge University Press; 2014:477-486.
Eye Movements
- Ask patient to keep their head still and follow a hatpin, pen, or your finger with their eyes, at a distance of approximately 30cm
- Move your finger in the following shape (Figure 3), to assess each of the extremes of movement
- Ask whether the patient is experiencing any pain, diplopia (‘double vision’), or visual blurring throughout the assessment
- Observe for any focal deficits in movement, or nystagmus
- Note: nystagmus at the extremes of vision can be normal

Figure 3. Schematic Diagram for Assessment of Eye Movements.
Pupils
- The 3 ‘S’s – size, symmetry, shape
- Anisocoria (different pupil sizes) occurs in at least 20% of people in the absence of any pathology, but may reflect an abnormally large pupil (e.g. CN II or CN III lesion), or an abnormally small one (e.g. in Horner’s syndrome)
- You may be guided by whether the anisocoria becomes more or less pronounced in light versus dark environments
- Irregularly shaped pupils are rarely normal, and may reflect inflammation (uveitis, iridocyclitis) or previous surgery/trauma
- Anisocoria (different pupil sizes) occurs in at least 20% of people in the absence of any pathology, but may reflect an abnormally large pupil (e.g. CN II or CN III lesion), or an abnormally small one (e.g. in Horner’s syndrome)
- Reflexes (best assessed in dim light)
- Light reflex
- Direct – pupil constricts when a pen-torch is shone into ipsilateral eye
- Consensual – contralateral pupil constricts when a pen torch is shone into the ipsilateral eye
- Relative Afferent Pupillary Defect (RAPD)
- Rapidly move pen torch between both eyes (i.e. ‘swinging light test’)
- If RAPD is present, the affected pupil will appear to dilate when light is shone into it due to lesion of direct pathway but intact consensual constriction
- Accommodation
- Ask the patient to focus on the wall behind you
- Hold a hatpin, pen, or your finger approximately 30cm away from their eyes in the midline
- Closely observing their pupils, ask them to focus on the close object, looking for bilateral and symmetrical constriction and convergence
- Light reflex
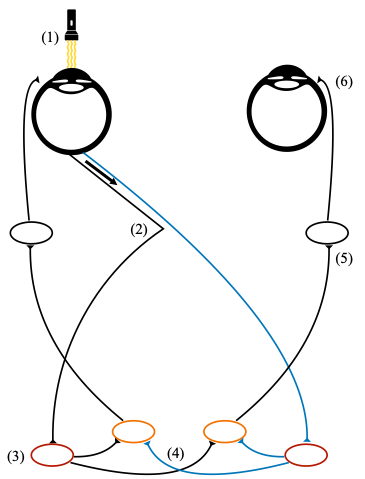
Figure 4. Schematic Diagram of the Pupillary Light Reflex. (1): Light shone into left pupil. (2): Optic nerve (CNII) fibres from the nasal retina cross to the contralateral (right) side at the optic chiasm, while temporal fibres remain uncrossed. (3): fibres from the left eye reach both the ipsilateral and contralateral pretectal nucleus (in red). (4): Interneurons from both pre-tectal nuclei synapse with both Edinger-Westphal nuclei (in orange). (5): EW nuclei each synapse with the ipsilateral ciliary ganglion (CNIII). (6): Each ciliary ganglion delivers nerve fibres via the short ciliary nerve to the ipsilateral pupillary sphincter.
Fundoscopy
- Please see our dedicated article on fundoscopy
Additional Tests
- It is pertinent to perform a full cranial nerve examination and consider whether the patient requires onward referral
- Several additional tests may be carried out if deemed necessary, but are not routinely performed in general medical environments
- Colour vision – in addition to colour blindness, may detect pathologies such as macular degeneration or certain cataracts
- Cover test – if any concern about strabismus, either a -phoria (latent squint) or -tropia (manifest squint)
- Further imaging – slit lamp, ultrasound, OCT, autofluorescence etc.
Author: Dr Archith Kamath BA BMBCh FHEA
Senior Editor: Mr Nachiketa Acharya MB BS, MD, FRCSEd (Ophth)