


Examination of the Cardiovascular System – detailed
Cardiovascular examination and questions for medical student exams, finals, OSCEs and MRCP PACES
Introduction
- Preparation
- Start by washing your hands
- Introduce yourself to the patient and obtain informed consent.
- Check the patient is not in any pain or discomfort and ensure he/she is positioned correctly, ideally with the chest fully exposed (this may cause embarrassment in female patients so one can try and access the auscultation points without full exposure but this may compromise the accuracy of the examination).
- The patient should be lying in bed with their upper body at 45 degrees and a pillow supporting the head.
General Inspection
- Begin the examination at the end of the bed with an inspection of the patient’s general condition and their surroundings.
- Explain to the patient what you are doing to avoid embarrassment. Although each anatomical area will be examined in detail later in the examination it is important to note signs such as dyspnoea, pallor or cyanosis which may be detectable at this stage.
- Note any medical equipment attached to the patient or in the bedspace
The Hands
Move to the left-hand side of the bed (the patient’s right side) and examine their hands.
- Begin by inspecting the finger nails for splinter haemorrhages and clubbing.
- Splinter haemorrhages are reddish-brown linear haemorrhages lying parallel to the long axis of the nail. They are a sign of previous trauma (classically gardening or mechanical work) or pathologically of infective endocarditis
- Clubbing is an enlargement of the soft tissue of the distal phalanges resulting in an exaggerated nail curvature, nail-fold bogginess and an angle of greater than 180° between the nail and nail-fold.
- Examine each of the fingers of each hand for these signs.
- Clubbing is an important sign but evidence suggests that it has poor precision. Schamroth’s sign may be a more reliable way to diagnose clubbing.
- Try to elicit Schamroth’s sign by asking the patient to curl the fingers of both hands towards the palms and then bring their hands together so the nails and distal interphalangeal joints of the two middle fingers touch.
- If clubbing is absent there should be a diamond shaped gap between the two nails. The loss of this gap is Schamroth’s sign and is an indicator of clubbing.
- Clubbing also occurs in the toe-nails but the toes are not routinely examined as part of the examination of the cardiovascular system.

Finger clubbing

Examining for Schamroth’s sign when looking for clubbing
- Examine the dorsum of the hands.
- Inspect along the extensor tendons for cholesterol deposits called xanthomata. These are irregularly-shaped, yellowish nodules on the skin.
- Then ask the patient to turn their hands over and examine the finger pulps for painful, red, raised nodules known as Osler nodes and the palms for flat, red macules known as Janeway lesions. These are both highly specific signs of infective endocarditis but they tend to present in the later stages of the disease and so are not commonly seen in the developed world.
- Note the temperature of the hands and the colour of the skin.
- Assess the patient’s peripheral perfusion by squeezing the fingertip firmly for five seconds then letting go and recording the time taken for normal colour to return. This is the capillary refill time and should be less than three seconds. A delay indicates poor perfusion of the extremities which may be caused by hypovolaemia, hypothermia, peripheral vascular disease or just cool peripheries (with associated vasoconstriction).
The Radial Pulse
- Palpate the right radial pulse by placing the tips of your index, middle and ring fingers over the radial artery, usually situated just medial to the radius.
- You should assess the rate, the rhythm and the character of the pulse.
- Establish the rate in beats per minute by counting the number of beats over a 15 second period and multiplying by four.
- The normal resting heart rate should be between 60 and 100 beats per minute.
- Then analyse the rhythm of the pulse and decide if it is regular, irregularly irregular, or regularly irregular.
- A regular pulse is at a constant frequency with a constant interval between the beats.
- If it is not of a constant frequency it is irregular.
- Irregular pulses are conventionally divided into ‘regularly irregular’ and ‘irregularly irregular’.
- A regular pulse is at a constant frequency with a constant interval between the beats.
- A regularly irregular pulse has a repeating pattern – for example two beats close together, then a gap and then another two beats close together.
- If there is no repeating pattern and the beats seem to arise randomly then the pulse is said to be irregularly irregular.
- A correlation of pulse character and underlying cardiac rhythm is beyond the scope of this article but one of the most common abnormalities of pulse rhythm is atrial fibrillation (AF) which gives an irregularly irregular pulse.
- The character of the radial pulse should also be assessed, although it is more accurate to do this in large volume central pulses such as the carotids.
- A ‘slow-rising’ pulse has a delayed up-stroke and occurs in aortic stenosis.
- A pulse is described as ‘bounding’ if it has an increased up-stroke and down-stroke. This may be a sign of CO2 retention.
- A ‘jerky’ pulse is characteristic of hypertrophic cardiomyopathy, but this is unlikely to be detected peripherally.
- Proceed to palpate both radial pulses simultaneously to detect any inequality in timing.
- This is known as radio-radial delay and is a sign of aortic coarctation.
- Check for inequality in the strength of the radial pulses.
- Strength inequality of arm pulses has been shown to be a highly sensitive sign in diagnosing aortic dissection.
- Examine for a collapsing pulse by placing your fingers across the anterior aspect of patient’s forearm and applying just enough pressure to occlude the radial pulse.
- Confirm that the patient has no pain in their shoulder, and then elevate their arm above their head whilst maintaining the position of your hand.
- You are feeling for a forceful knocking sensation that is typical of aortic regurgitation, commonly known as the ‘collapsing’ or ‘water-hammer’ pulse.
- Radio-femoral delay is the sign that is present if the femoral pulse comes after the radial pulse. The two pulses should occur at the same time and radiofemoral delay is a sign of coarctation of the aorta.
- The difficulty exposing the femoral artery means that this part of the examination is not included in routine cardiovascular examinations.
- In OSCEs you should simply indicate to the examiner that at this point you would like to palpate for radio-femoral delay. See Examination of the Peripheral Arterial System.

Examining for a collapsing pulse
Blood Pressure
- Measure the patient’s arterial blood pressure using a spyhgnomanometer. In an OSCE, it is unlikely you will have the time to actually measure it but it is an essential part of the cardiovascular examination and you must indicate this to the examiner at this point.
- Ensure the cuff is the appropriate size for the patient. An undersized cuff will overestimate the ABP and vice versa.
- Ensure the patient is comfortable and support their arm at around heart level.
- Wrap the cuff around the upper arm, palpate the radial artery and then inflate the cuff until the radial pulse can no longer be detected. The pressure at which the pulse is lost gives a rough estimate of the systolic blood pressure.
- Deflate the cuff and place your stethoscope over the brachial artery which is situated in the antecubital fossa, just medial to the biceps tendon, midway between the medial and lateral epicondyles of the humerus.
- Reinflate the cuff to around 20mmHg above the estimated systolic blood pressure and then deflate it slowly (2-3mmHg per second) until a sound is first heard over the artery (Korotkoff 1). The pressure at which this occurs is the systolic blood pressure.
- Continue to deflate the cuff until the sounds disappear (Korotkoff V). The pressure at which this occurs is the diastolic blood pressure.
- Normal arterial blood pressure is defined as systolic blood pressure of less than 140mmHg and diastolic blood pressure of less than 90mmHg. Having measured the arterial blood pressure go on to
calculate the pulse pressure which is the difference between the systolic blood pressure and the diastolic blood pressure. The pulse pressure may be narrow in aortic stenosis and wide in aortic regurgitation.
Postural Blood Pressure
- A full examination of the cardiovascular system should include lying and standing blood pressure to see if there is a postural drop in blood pressure. But this should not be done at this stage in a medical school examination because there is not sufficient time. Simply indicate to the examiner that you would like to perform it and mention it again at the end of your examination.
- To measure the postural blood pressure, position the patient lying supine, wait two minutes then measure the blood pressure as described above.
- Then stand the patient up, wait a further minute and repeat the blood pressure reading.
- A postural drop in blood pressure is defined as a fall on standing of greater than 15mmHg in systolic BP or 10mmHg diastolic.
Face, Eyes and Mouth
- Look around the eyes for yellow cholesterol deposits known as xanthelasma.
- These are sharply demarcated, yellow plaques, usually around 1-2mm and most commonly found on the upper and lower eyelids.
- Examine the iris for senile arcus, a grey or white arc visible around the cornea.
- These are signs of hyperlipidaemia.
- Ask the patient to look up, and retract the lower eyelid to inspect for conjunctival pallor which is a sign of anaemia.
- Use a pen-torch to examine the inside of the mouth. Inspect below the tongue and the lips for central cyanosis, a blue discolouration of the skin and mucous membranes as a result of hypoxia.
- Inspect the mucosa for petechiae which can be caused by infective endocarditis and note the patient’s dental hygiene. Poor dental hygiene is a risk factor for infective endocarditis.
The Neck
- Examination of the neck includes assessment of the jugular pulse and the carotid pulse.
The Jugular Venous Pulse
- The jugular venous pulse (JVP) provides an estimate of the central venous pressure (CVP) and hence the patient’s volume status and heart function. Although it is an important part of the examination, clinical assessment of CVP using the JVP has poor sensitivity.
- To assess the JVP, ask the patient to turn their head to the left and extend their neck directly backwards. It may be helpful to gently move the patient’s head into the correct position.
Video on how to examine the JVP
- First measure the height of the JVPs highest point in centimetres. This is the vertical height above the sternal angle at which a pulsation is observed in the internal jugular vein.
- It is very important that the patient is positioned at 45° because this angle directly influences the height of the JVP for any given CVP.
- Look for the JVP along the course of the vein which travels from the earlobe, down the neck and into the chest, between the two heads of sternocleidomastoid. A JVP of greater than 4cm is said to be elevated.
- It may be difficult to distinguish the JVP from the carotid pulse but there are a number of differentiating features that will help you make the distinction.
- Make an assessment of the waveform of the JVP. Figure 1 of Levick & Dwight shows the normal waveform.
- Simultaneously palpating the contralateral carotid may help you in identifying its different components.
- The a-wave coincides with the first heart sound and precedes the carotid pulse.
- Go on to try and elicit hepatoojugular reflux. Ensure the patient has no abdominal pain and press firmly on their right upper quadrant for 15-30 seconds and inspect the JVP.
- A sustained increase of 4cm or greater throughout the compression is a sign of right ventricular failure.
- Ask the patient to breathe slowly through the mouth, then look for the presence of Kussmaul’s sign: a paradoxical increase in the JVP with inspiration.
- This can occur in any condition where right ventricular filling is restricted such as constrictive pericarditis or cardiac tamponade.
The Carotid Pulse
- Palpate the carotid artery, medial to the sternocleidomastoid, paying particular attention to its character and volume, as well as the rate and rhythm. Palpate each side in turn, never simultaneously as this may compromise the cerebral blood supply.
The Precordium
Inspect
- Begin by inspecting for scars.
- Look at the midline of the chest for a median sternotomy scar which would indicate previous valve surgery or a coronary artery by-pass graft.
- Examine the mid-axillary lines for a lateral thoracotomy scar indicating previous thoracic surgery.
- Look under the clavicles for a cardiac pacemaker or defibrillator.
- Look for visible cardiac impulses.
Palpate
- Palpate the apex beat first.
- The apex beat is defined as the most lateral and inferior point on the chest wall at which a cardiac impulse can be felt.
- To locate it, identify the sternal angle found at the junction of the sternum and second rib, move your fingers laterally and inferiorly to the second intercostal space, then count down the intercostal spaces in the midclavicular line.
- The apex beat should be situated in the fifth intercostal space along the midclavicular line.
- If the apex beat is impalpable here, move inferiorly and laterally.
- Displacement of the apex in this direction suggests cardiomegaly.
- Go on to assess the character of the apex beat.
- Decide if it is normal, pressure-overloaded or volume-overloaded.
- A pressure-overloaded apex is heaving, sustained and forceful, and develops as a result of aortic stenosis or hypertension.
- A volume-overloaded apex is diffuse and displaced laterally and/or inferiorly.
- This may be a feature of aortic or mitral regurgitation, dilated cardiomyopathy or ventricular damage due to ischaemic heart disease.
- A ‘tapping’ apex beat is a palpable first heart sound and a sign of mitral stenosis.
- A ‘double impulse’ apex (two beats per cardiac cycle) is a sign of hypertrophic cardiomyopathy.
- Place the heel of your hand over the lower left sternal edge and feel for a right ventricular heave as a push against your hand. This is a sign of right ventricular hypertrophy.
- Then feel for thrills by systematically placing the flat of your hand over the apex (mitral valve area), lower left sternal edge (tricuspid valve area), right 2nd intercostal space (aortic valve area) and left 2nd intercostal space (pulmonary valve area).
- Decide if it is normal, pressure-overloaded or volume-overloaded.
Video on how to examine the apex beat, heaves and thrills
Auscultate
- Positions
- Begin auscultation of the heart by listening over the four valve areas shown in the figure below with the diaphragm of the stethoscope.
- Auscultate in the following order:
- mitral
- tricuspid
- aortic
- pulmonary
- Then auscultate over both carotid arteries and the left axilla to detect the radiating murmurs of aortic stenosis and mitral regurgitation respectively.
- Listen over each carotid using the bell whilst the patient comfortably holds a breath.
- Auscultation over the carotids also allows for the detection of a stenotic carotid bruit which can be distinguished from a radiating murmur by identifying the site of the sound’s maximal intensity; the former heard loudest above the thyroid cartilage, the latter over the precordium.
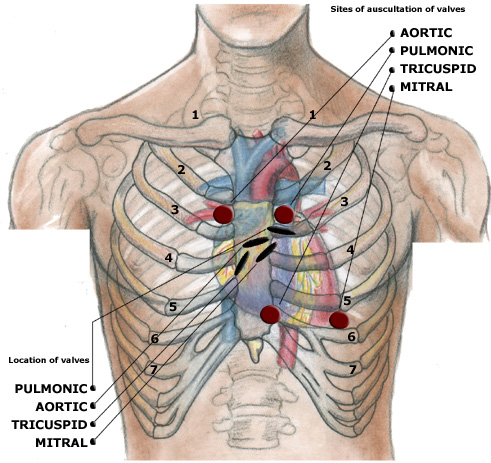
The four auscultatory areas
- Heart Sounds
- During auscultation you should listen for the following at each valve position: first and second heart sounds (S1 and S2), added heart sounds and murmurs.
- S1 and S2
- When auscultating the valve areas, start by identifying the first (S1) and second (S2) heart sounds which are caused by the closure of the atrioventricular and semi-lunar valves respectively.
- Simultaneously palpating a peripheral pulse (the radial is often the most convenient) will help to distinguish systole and diastole.
- S1 marks the start of systole and coincides with the peripheral pulsation. Physiological splitting of S2 is common, and characteristically increases at end-inspiration but wide splitting (exaggerated physiological splitting), fixed splitting (unaffected by respiration) and reverse splitting (widens in expiration) all have underlying pathologies.
- Added Sounds
- Now listen between S1 and S2 for added heart sounds.
- The 3rd heart sound (S3) is a low-pitched extra heart sound that occurs in early diastole, just after S2, and is best heard over the apex. It produces a ‘gallop’ rhythm often compared to the cadence of the word ‘Kentucky’ with the syllables ‘ken’, ‘tuc’ and ‘ky’ representing S1, S2 and S3 respectively.
- The presence of the third heart sound may indicate left ventricular failure, mitral regurgitation or high output cardiac states, but it can be physiological in the young.
- Listen for a fourth heart sound (S4), which is slightly higher-pitched and occurs in late-diastole, immediately before S1. It produces a ‘gallop’ rhythm often compared to the cadence of the word ‘Tennessee’ with the syllables ‘ten’, ‘nes’ and ‘see’ representing S4, S1 and S2 respectively.
- A fourth heart sound is indicative of a poorly compliant ventricle and is always pathological, associated with aortic stenosis, hypertension and left ventricular failure.
- Go on to auscultate for other abnormal sounds. First, listen for an ejection click, a high-pitched ringing sound heard in early systole shortly after S1. This is a feature of aortic or pulmonary stenosis and is thought to be caused by the sudden opening of the deformed valve. Listen for a mid-systolic click, a sound most often associated with mitral valve prolapse which may be accompanied by a late systolic murmur. Listen in early diastole for an opening snap heard in mitral stenosis. This is best heard over the lower left sternal edge and is caused by the rapid opening of a stenosed but pliable mitral valve under high left atrial pressure.
- Finally, listenthroughout the cardiac cycle for the ‘walking on snow’ sound of a pericardial friction rub, caused by pericarditis.
- The 3rd heart sound (S3) is a low-pitched extra heart sound that occurs in early diastole, just after S2, and is best heard over the apex. It produces a ‘gallop’ rhythm often compared to the cadence of the word ‘Kentucky’ with the syllables ‘ken’, ‘tuc’ and ‘ky’ representing S1, S2 and S3 respectively.
- Now listen between S1 and S2 for added heart sounds.
- Murmurs
- Murmurs should be considered in terms of timing, site of greatest intensity, character, loudness, and
radiation. - The intensity of a murmur does not really help in assessing the severity of the valve lesion, but a change in intensity may be of importance. Murmur intensity can be quantified using Levine’s grading system. Of all the features of a murmur, its timing is most important diagnostically.
- Murmurs should be considered in terms of timing, site of greatest intensity, character, loudness, and
Auscultate with Manoeuvres
- Murmurs are accentuated by the position of the patient during auscultation and the following manoeuvres should be performed as part of the routine examination.
- Ask the patient to turn onto their left hand side. Ensure they are comfortable then ask them to hold their breath in expiration.
- Auscultate the apex with the bell. You are listening for the accentuated mid-diastolic murmur of mitral stenosis.
- Then ask the patient to sit forward. Ensure they are still comfortable and again ask them to hold their breath in expiration.
- Auscultate over the lower left sternal edge with the diaphragm. You are listening for the accentuated early diastolic murmur of aortic regurgitation.
- Whilst expiration accentuates left-sided murmurs, inspiration accentuates right-sided murmurs. This can be remembered because RIGHT has an ‘I‘ (inspiration) in it and LEFT has an ‘e‘ (expiration) in it.
- and this may help in distinguishing the pan-systolic murmurs of mitral and tricuspid regurgitation. A pansystolic murmur that increases in intensity in expiration is most likely due to mitral regurgitation whereas one that increases in inspiration is mostlikely due to tricuspid regurgitation.
The Back, Abdomen and Legs
- Ask the patient to lean forwards.
- Percuss the lung bases for a pleural effusion and auscultate for fine inspiratory crackles (signs of heart failure).
- Check for sacral oedema by placing one finger firmly on the sacrum for ten seconds and observing for the persistence of an indentation after release.
- Examine the ankles for pedal oedema by placing one finger firmly on the ankle for five seconds and observing for the persistence of an indentation after release.
- If present, repeat the procedure at regular points on the legs moving upwards towards the knees. Note the point on the leg to which the oedema extends.
Completing the Examination
- Thank the patient, help them back into comfortable posture and wash your hands.
- Give the patient some privacy to redress.
- In an OSCE you should finish by addressing the examiner, stethoscope behind your back, not looking back at the patient. See here for a summary.
- To present, reiterate the manouevres you mentioned during the examination but did not perform. These will include examination of the toenails, examining for radio-femoral delay, and measuring postural blood pressure. You should also indicate your desire to examine the peripheral pulses as detailed in the Examination of the Peripheral Arterial System and to examine the abdomen for an abdominal aortic aneurysm and an enlarged liver (heart failure). Go on to explain the special tests and bedside investigations you would like to undertake, as detailed below.
Pulsus paradoxus
- Pulsus paradoxus is usually defined as an inspiratory decline in systolic BP that exceeds 10mmHg, but a more appropriate threshold may be 12mmHg which has been shown to be the upper 95% confidence interval for an inspiratory drop in normal individuals.
- It occurs in 98% of patients with cardiac tamponade and is a highly sensitive and specific sign in identifying the condition in those with known pericardial effusions.
- One should therefore always check for pulsus paradoxus in patients with suspected pericardial disease and you should indicate this to the examiner.
- To measure pulsus paradoxus, begin by measuring the BP as described but on hearing the first Korotkoff sound, prevent further deflation of the cuff. In patients with paradox, the sounds are intermittent with respiration. Note this pressure then continue to deflate the cuff until sounds are heard throughout the respiratory cycle. The amount of paradox in mmHg is the difference between the pressure at this point and the initial measurement.
Bedside Investigations
- Routine observations are an essential part of the cardiovascular exam.
- You have already calculated the heart rate and BP. You also need to know the respiratory rate, the oxygen saturations and the temperature of the patient.
- An ECG should be checked for signs of ischaemia or arrhythmia
- Uninalysis is indicated if endocarditis is suspected
- An echocardiogram is indicated if there is suspicion of structural or valve disease
- Questions about the cardiovascular exam
- What are the causes of clubbing?
- What are the causes of atrial fibrillation?
- What are the factors to distinguish the jugular venous from the carotid arterial pulse?
- What are the abnormalities of the waveform of the jugular venous pulsation?
- What are the different murmurs and clinical findings in the common valvular lesions?
- What are the abnormalities of the heart sounds (relevance of 1st, 2nd, 3rd and 4th heart sounds)?
- What are the grades of murmur intensity (Levine scale)?
- What is the differential diagnosis of differently timed murmurs?
- Cardiovascular examination evidence
Click here for medical student OSCE and PACES questions about Examination of the Cardiovascular System
Common Examination of the Cardiovascular System exam questions for medical students, finals, OSCEs and MRCP PACES