


Pneumothorax
Definition of a pneumothorax
- Air in the pleural space leading to lung deflation. Pneumothoraces can be divided into:
- Primary: otherwise “normal” lung
- Secondary: underlying lung disease e.g. COPD
- Tension: mediastinal shift and respiratory compromise
Epidemiology of pneumothoraces
- Approximately 10 per 100,000
- Male>Female (6:1)
- > 40 years often associated with COPD
- Smoking increases the risk of pneumothorax
Causes of pneumothoraces
- Spontaneous/ Primary
- Thought to be due to congenital weakness of a pleural bleb
- Secondary
- COPD, Asthma, Lung cancer, Pulmonary Fibrosis, TB, Sarcoid, CF, PCP
- Marfans, Ehlers Danlos, Psuedoxanthoma elasticum
- Iatrogenic
- Pleural aspiration or biopsy
- CVP or pacemaker insertion
- CPR
- Chest trauma
- Penetrating chest injury
- Tension pneumothorax is more likely in this group
- Penetrating chest injury
- Intubation and ventilation
- Especially with high pressures used
Presentation of a pneumothorax
- Pleuritic chest pain and shortness of breath
- (but note may be asymptomatic)
- Signs:
- Tachycardia and tachypnoea
- Cyanosis
- Tracheal deviation
- Hyper-resonance to percussion
- Decreased breath sounds
- In tension pneumothorax:
- Raised JVP, pulsus paradoxus, marked tracheal deviation, Tachycardia >135, hypotension, distended neck veins
https://www.youtube.com/watch?v=j_UGBS-Kp2I
Differential diagnosis of a pneumothorax
- Pleural effusion
- PE
- Pneumonia
- Pericarditis
Investigation of a pneumothorax
- ABG
- Hypoxia, severity dependent on size of pneumothorax and respiratory reserve
- CXR
- Will show characteristic rim around outside of lung
- Size can be estimated by depth of rim at hilum
- 2cm is approximately equal to 50% lung volume lost
- In supine films, look for deep costophrenic sulci, darkened lung field and prominent heart border.
- USS Chest
- Can be helpful to look for iatrogenic pneumothorax following US guided drain insertion/ pleural biopsy
- CT
- Can detect occult pneumothoraces
- Can be useful to differentiate bullae from pneumothorax
- To look for causes of persistent leak in patients with non-resolving pneumothorax
Staging of pneumothorax
- Small vs Large
- > 2cm rim between lung margin and chest wall at the level of the hilum
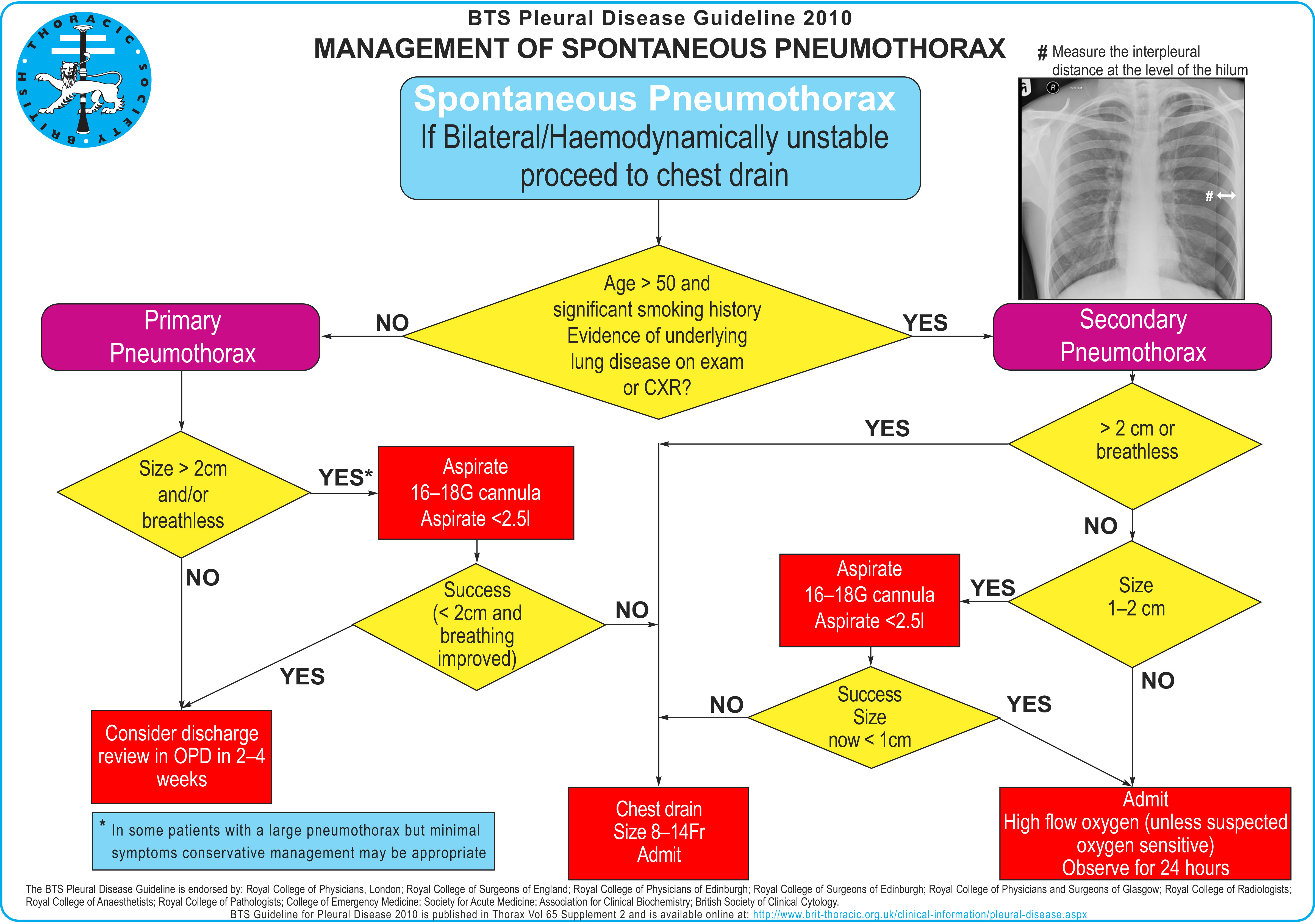
Management of a pneumothorax
- Observation In small primary pneumothorax without significant shortness of breath.
- Patients with primary or secondary pneumothorax and significant breathlessness should undergo active intervention
- Supportive oxygen therapy
- Needle aspiration or chest drain (see BTS algorithm below)
- See page on pleural drain here and pleural aspiration here
- Suction
- High volume low pressure suction systems
- Risk of re-expansion pulmonary oedema
Further management of a pneumothorax
- Surgical
- Those with persistent air leak at 48 hours should be discussed with thoracic surgeons.
- Surgical management options include:
- Open thoracotomy and pleurectomy (give lowest recurrence rates)
- VATs with pleurectomy and pleural abrasion (better tolerated)
- Surgical chemical pleurodesis
- Medical pleurodesis
- Considered for patients refusing/ not fit enough for surgery
- Ambulatory management with Heimlich valve
- Smoking cessation
Treatment of tension pneumothorax (a medical emergency):
- High-flow oxygen
- Emergency needle decompression
- Large cannula, second intercostal space (just above third rib), mid-clavicular line
- Converts tension to a simple pneumothorax
- Followed by chest drain insertion for definitive management
Complications of pneumothoraces
- Respiratory failure
- Conversion to tension pneumothorax
- Bronchopleural fistula
- Recurrence
Prognosis in pneumothorax
- Good if treated but recurrence is common: up to 30% overall.
- Mortality low, but increased in secondary versus primary pneumothorax
Click here for medical student OSCE and PACES questions about Pneumothorax
Common Pneumothorax exam questions for medical students, finals, OSCEs and MRCP PACES
Click here to download free teaching notes on Pneumothorax: Pneumothorax; BTS guidelines for pneumothorax
Perfect revision for medical students, finals, OSCEs and MRCP PACES