


Skin Examination
How to examine the skin. A system for doctors, medical student finals, OSCEs and MRCP PACES
Introduction
- Skin complaints are common in clinical exams and everyday practice
- Skin cancers are increasing in prevalence and – if detected early – treatment may be curative
- Cutaneous signs can also be vital in identifying systemic diseases
- With a structured examination technique and a little knowledge of terminology (see below), skin signs can be described and classified systematically
Preparation (WIIPPPPE)
- Wash your hands
- You should wear gloves if the condition is weeping or likely to be contagious
- Introduce yourself
- Identity of patient (confirm)
- Permission (consent and explain examination)
- Pain?
- Privacy
- Exposure
- Remember that some conditions require access to certain areas (e.g. the elbows and scalp in psoriasis; the soles in palmoplantar pustular psoriasis)
Before examining, remember how you will try to describe the lesions…
How to describe skin lesions
| Lesion | Description | Example |
|---|---|---|
| Primary Lesions | ||
| Macule | <0.5cm, flat, circumscribed area of altered skin colour | Vitiligo (small) |
| Patch | ≥0.5cm, flat, circumscribed area of altered skin colour | Vitiligo (large) |
| Papule | <0.5cm, circumscribed elevation of skin | Molluscum contagiosum |
| Plaque | ≥0.5cm, circumscribed elevation of skin | Psoriasis |
| Weal | Transient, smooth, slightly raised lesion, characteristically with a pale centre and a pink margin | Urticaria |
| Vesicle (blister) | <0.5cm, circumscribed, fluid-containing elevation | Acute eczema e.g. pompylox |
| Bulla (blister) | ≥0.5cm, circumscribed, fluid-containing elevation | Burn, friction |
| Pustule | Visible collection of pus | Staphylococcal folliculitis |
| Abscess | Localised collection of pus in a cavity | Bacterial infection |
| Erythema | Redness, blanching | Erythema nodosum |
| Purpura | Redness, non-blanching, secondary to collections of red blood cells | Vasculitis, platelet or clotting defect |
| Telangiectasis | Dilated capillaries visible on the skin surface | Side-effect of topical steroids |
| Secondary Lesions | ||
| Scale | Thickened, loose, readily detached fragments of stratum corneum | Psoriasis |
| Crust | Dried exudate | Impetigo |
Also consider how you will describe the distribution of lesions…
 Position of skin lesions
Position of skin lesions
Inspection
- Before starting
- Some lesions may be seen more easily with side-lighting than direct illumination. A supplementary adjustable light source is therefore useful
- Cover sensitive areas such as breasts and genitalia once they have been inspected
- At the bedside
- Check the bedside for tubes of ointment or tubs of emollient (are they being used?)
- What is prescribed on the drug chart (many rashes are caused by drugs) and is it being taken?
- The patient
- General
- Does the patient look well? Is he/she scratching or displaying other signs of distress?
- Inspection should include the nails, the scalp, the hair and the mucous membranes (inside the mouth)
- Basics of rash description
- Distribution (symmetry)
- Is it symmetrical suggesting a systemic (endogenous) aetiology or asymmetrical suggesting an external cause e.g. infection, trauma, contact dermatitis?
- Does the rash involve particular sites e.g. extensor or flexural, sun-exposed or covered?
- Do lesions adopt any particular pattern e.g. diffuse, linear, grouped or scattered (see below)?
- Examine scars as some problems arise in previously damaged skin (the Koebner phenomenon).
- Colour
- What colour is the affected skin – red, purple, brown?
- Do lesions leave pigment change (increased or decreased) or scars?
- Shape and size
- Border
- Is the border well-demarcated or indistinct?
- Ask the patient to indicate early and late lesions.
- Decide what is primary or secondary and how lesions evolve or spread.
- Distribution (symmetry)
- Specifics of rash description
- Excoriation
- Look for linear scratch marks (excoriations) indicative of itching (pruritus)
- Ulcer/erosion
- Is the skin eroded (superficial epidermal loss) or ulcerated (dermal damage)?
- Weeping
- Crusting, hyperkeratosis or scale
- Blood vessels
- Are blood vessels easily visible suggesting skin atrophy or increased superficial vasculature (telangiectasia)?
- Odour
- Foul-smelling ulcers may be infected with anaerobes or Pseudomonas aeruginosa. Some rashes smell unpleasant e.g. Darier disease
- Excoriation
- General
Descriptive terms for the shape of skin lesions
| Terminology | Pattern of lesions |
|---|---|
| Grouped |  |
| Linear |  |
| Serpiginous (wavy) |  |
| Arcuate (curved) |  |
| Nummular/discoid (coin like) |  |
| Annular (ring-like) |  |
Palpation
- Tenderness (ask the patient first!)
- In the elderly, patients taking systemic steroids or patients with rheumatoid arthritis, the skin may exceptionally fragile
- Surface texture
- The surface texture of lesions can be assessed by running a finger over the top of a lesion to feel if the skin is smooth or rough (hyperkeratotic)
- Scaling
- If scaling is not easily visible, lightly scrape a lesion with your fingernail to establish whether there is any scaling (indicating epidermal involvement)
- Elevation
- Are lesions raised (palpable) or flat or does the patient have both raised and flat lesions (a maculopapular rash)?
- If the skin is red:
- Check if this is an erythema (blanching with light pressure)
- Purpura (nonblanching) is caused by leakage of blood into the perivascular dermal tissues
- Flat purpura suggests leakage without inflammation and may be indicative of inadequate dermal elastic tissue e.g. atrophic elderly or sun damaged skin or a coagulation disorder
- Palpable purpura suggests associated inflammation and is likely to be caused by a small-vessel cutaneous vasculitis such as Henoch-Schonlein purpura
- Skin thickness and depth of involvement
- Is there any atrophy (tissue loss) with wrinkling or dimpling (loss of fat)?
- Does the problem involve the dermis or do you think it extends more deeply into the fat (panniculitis)?
- Press gently to assess the firmness of lesions to distinguish between solid lesions and those that are filled with fluid
- Tethering
- Gently pinch the skin or try to pick up lumps between finger and thumb to assess depth. Is there any tethering to underlying tissues?
- Check for associated signs
- Feel the temperature of involved skin and compare with normal
- Inflamed skin e.g. cellulitis is hot while poorly perfused skin is cold
- Is there extending erythema associated with oedema or crepitus
- Crepitus is the sound produced when palpating skin with bubbles of gas beneath. This can indicate necrotising fasciitis or gas gangrene
- Feel the temperature of involved skin and compare with normal
Examining Pigmented Lesions
- Skin cancer is the commonest cancer and any examination of the skin should include a check for sun damage and potential skin malignancy
- Malignant melanoma must be distinguished from more common pigmented lesions such as:
- Seborrhoeic warts (common in the elderly)
- “Sunspots” (solar lentigines)
- Benign melanocytic naevi (moles)
- The “ugly duckling” sign may help when examining patients with many melanocytic naevi (moles): a “mole” that stands out and looks very different from the surrounding moles should be checked particularly carefully to exclude malignancy
- Two methods have been advanced to assist in diagnosing malignant melanoma: ABCD(E) and the revised 7-point checklist
Diagnosing melanoma - the ABCDE and revised 7-point system
| ABCD(E) system | Revised 7-point checklist |
|---|---|
| Asymmetry | Major criteria (2 points each) |
| Border irregularity | Change in size |
| Colour variation | Change in shape |
| Diameter >6mm | Change in colour |
| Evolution over time | minor criteria (1 point each) |
| Inflammation | |
| Crusting/bleeding | |
| Sensory change | |
| Diameter ≥7mm | |
| Refer to a dermatologist if a lesion has ≥1 of the above | Refer to a dermatologist if a lesion scores ≥3 points |
Any patient with a suspicious lesion should be seen by a dermatologist who may extra equipment (e.g. a dermatoscope) to assess it further…
Extra Equipment
- Wood’s Light
- A Wood’s light emits UVA radiation and accentuates some forms of hypo- or hyperpigmentation
- Wood’s light also detects some skin infections e.g. erythrasma fluoresces coral red, some fungal infections glow green
- Dermatoscopes
- Dermatoscopes magnify skin signs such as nail fold capillaries or scabies burrows but are most often used to differentiate benign from malignant pigmented lesions
- Features that indicate malignancy include irregular dots of pigment, irregular peripheral extensions of the lesion (pseudopods) and a blue-white veil around the periphery of the lesion
- Dermatoscopes magnify skin signs such as nail fold capillaries or scabies burrows but are most often used to differentiate benign from malignant pigmented lesions

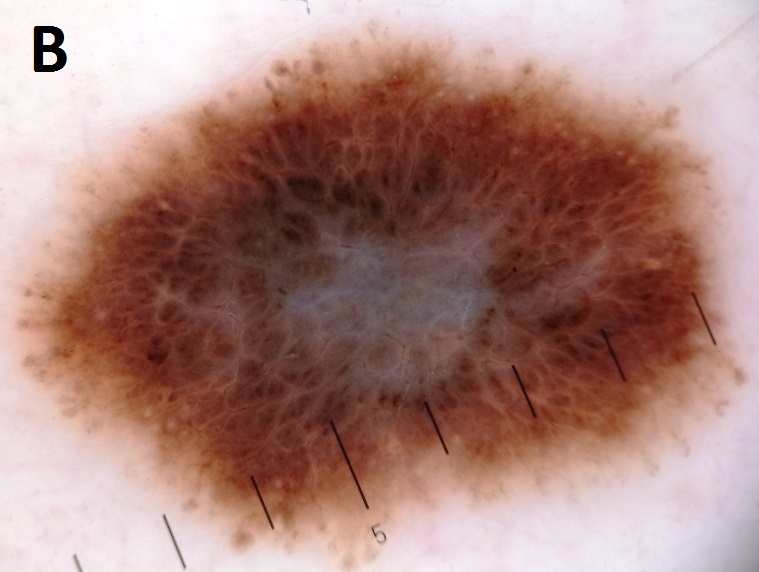
Views of a melanoma with the unaided eye (A) and with a dermatoscope (B) showing irregular dots of pigment, irregular peripheral extensions (pseudopods) and a blue-white veil [the scale shown is in millimetres]
Complete the examination
- Thank the patient after finishing the examination
- Make sure they are comfortable and happy getting dressed
- Wash or use alcohol gel on your hands
- Turn to the examiner to present your findings…
Summary of skin examination
- Inspection
- Around the bedside
- The patient
- Basics of rash description
- Site; shape; size; symmetry
- Colour
- Border
- Specifics
- Excoriation
- Ulcer/erosion
- Weeping
- Crusting, hyperkeratosis or scale
- visibility of blood vessels
- Odour
- Basics of rash description
- Palpation
- Tenderness (ask the patient first!)
- Surface texture
- Elevation
- Skin thickness
- Blanching
- Tissue loss
- Tethering
- Associated signs
- Temperature
- Oedema
- Crepitus
- Extra tests
- Wood’s lamp
- Dermatoscopy
- Thank the patient
Click here to learn about the hand examination and here for the lump and bump examination
Perfect revision for medical student finals, OSCES and PACES