


Common respiratory examination exam questions for medical finals, OSCEs and MRCP PACES
Click on the the example questions below to reveal the answers
Question 1.
What is the surface anatomy of the lungs?
The surface anatomy of the lungs is shown below. The lungs are shown in mid-inspiration. 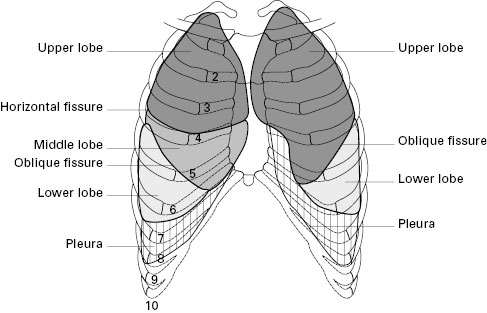
Question 2.
What are the respiratory causes of clubbing?
- Fibrotic lung disease
- Chronic suppurative lung disease (bronchiectasis, chronic lung abscesses)
- Lung cancer (all except small cell which tends to progress too fast to induce clubbing)
NB. COPD does not cause clubbing. If a COPD patient has clubbing look for co-existing pathology
Question 3.
How do you examine for tracheal deviation?
- Placing your index and ring finger of the right hand on the head of each clavicle, use the middle finger of the same hand to palpate the trachea in the sternal notch. Roll you finger across the trachea in the horizontal plane to assess for deviation.
Question 4.
What is the cricosternal distance and tracheal tug?
- The cricosternal distance is the distance between the inferior border of the cricoid cartilage and the sternum.
- To measure it, put the index finger of your right hand on the patient’s trachea against the inferior edge of the cricoid cartilage. Place subsequent fingers, in the vertical plane, below this into the sternal notch until the trachea is no longer palpable and the sternum is reached.
- This is the crico-sternal distance and is normally three finger widths (5cm) or more. Note whether the trachea moves inferiorly, reducing the crico-sternal distance on inspiration, referred to as tracheal tug.
- A reduction in the crico-sternal distance and tracheal tug signify marked chest hyperexpansion, usually COPD.
Question 5.
What are the common causes of decreased chest expansion?
- Reduced chest expansion may be secondary to fibrosis, consolidation, effusion, collapse or pneumothorax.
- Unilaterally decreased expansion is a useful finding as the pathology is invariably on the side of decreased expansion
Question 6.
What are the common causes of wheeze?
- Obstructive lung diseases, particularly COPD or asthma
Question 7.
What is stridor and what does it indicate?
- Stridor is a high-pitched, monophonic breath sound, usually occurring in inspiration.
- It results from turbulent air flow in the larynx or lower in the bronchial tree and implies obstruction at these (upper airway) levels.
Question 8.
What are the causes of dullness to percussion on respiratory examination?
- Effusion
- Consolidation
- Lobectomy or pneumonectomy
- Raised hemidiaphragm
- Pleural thickening
Question 9.
How do you differentiate consolidation and pleural effusion clinically?
- Both are dull to percussion (though effusion is classically ‘stony dull’)
- In effusion vocal resonance is decreased or absent, in consolidation vocal resonance is increased
Question 10.
How do you differentiate a transudative from an exudative pleural effusion?
- Transudate
- Protein <30 g/l: in patients with normal serum protein
- Exudate
- Protein >30 g/l: in patients with normal serum protein
- Light’s criteria
- More sensitive for diagnosis of exudative effusions and helpful if fluid protein between 25-35 g/l. Positive if one of these is true:
- Pleural:serum protein ratio; >0.5 = exudate
- Pleural:serum LDH ratio; >0.6 = exudate
- Pleural LDH >2/3 the upper limit of normal serum LDH
- More sensitive for diagnosis of exudative effusions and helpful if fluid protein between 25-35 g/l. Positive if one of these is true:
Question 11.
What are the causes of fibrosis?
Click here for mnemonics on how to remember the causes of fibrosis.
A more logical system is shown below:
- Usual interstitial pneumonia (UIP)
- Also called Idiopathic Pulmonary Fibrosis (IPF) and Cryptogenic Fibrosing Alveolitis (CFA)
- Occupational
- Asbestosis
- Silicosis
- Pneumoconiosis
- Extrinsic Allergic Alveolitis (EAA)
- Rheumatological
- Rheumatoid arthritis; SLE; dermatomyositis; polymyositis; Sjogrens; anklylosing spondylitis; systemic sclerosis
- Infection
- Aspergillosis (ABPA)
- TB
- Drugs
- Amiodarone
- Methotrexate
- Bleomycin
- Cyclophosphamide
- Nitrofurantoin
- Vasculitis
- Wegeners; Churg-strauss; Goodpastures
- Radiation fibrosis
- Recurrent aspiration
- Sarcoid
- Histiocytosis
Click here for all the clinical examinations: how to examine, what to look for and how to present your findings