


Cardiac Arrest
Initial management of cardiac arrest
- On finding an unconscious individual, follow the three SSS’s: safety, shake, shout
- Safety: ensure it is safe to approach
- Shake: ask the patient “Are you alright?” whilst shaking their shoulder
- Shout: if the patient responds, assess them from an ABCDE perspective; if they do not respond, shout for help and put out a cardiac arrest call
- Open the airway with a head tilt/chin lift manoeuvre, palpate the carotid pulse and look, listen and feel for breathing for 10 seconds
- If there is a risk of a cervical spine injury, open the airway using a jaw thrust whilst an assistant applies manual in-line stabilisation (MILS)
- If there is no pulse, no signs of life, or if in any doubt, commence cardiopulmonary resuscitation (CPR) immediately in a ratio of 30 compressions to 2 ventilationcompressions should be applied to the lower half of the sternum to a depth of 5-6 cm at a rate of 100 per minute
- Ventilations should ideally be applied via a bag-valve-mask (BVM) attached to an oxygen supply, but if these are unavailable can be given via a pocket mask or mouth-to-mouth
- Attach defibrillator pads and pause CRP to analyse the rhythm; further management will depend of whether the rhythm is shockable (ventricular fibrillation [VF] or pulseless ventricular tachycardia [VT]) or non-shockable (asystole or pulseless electrical activity [PEA])
Management of shockable rhythms (VF and pulseless VT)
- On recognising a shockable rhythm, resume chest compressions immediately
- First shock
- Warn all other individuals to stand clear and remove any oxygen delivery device whilst the defibrillator is charged to 150 J (this is the value on most machines, check local protocols)
- Once the defibrillator is charged, instruct the individual performing chest compressions to stand clear and then deliver the first shock
- Resume CPR immediately and continue for two minutes
- After two minutes, pause CPR to check the rhythm; on recognising a shockable rhythm, resume chest compressions immediately
- Second shock
- Warn all other individuals to stand clear and remove any oxygen delivery device whilst the defibrillator is charged to 150 J
- Once the defibrillator is charged, instruct the individual performing chest compressions to stand clear and then deliver the second shock
- Resume CPR immediately and continue for two minutes
- After two minutes, pause CPR to check the rhythm; on recognising a shockable rhythm, resume chest compressions immediately
- Third shock
- Warn all other individuals to stand clear and remove any oxygen delivery device whilst the defibrillator is charged to 150 J
- Once the defibrillator is charged, instruct the individual performing chest compressions to stand clear and then deliver the third shock
- Resume CPR immediately and continue for two minutes
- Medications
- After the third shock, give adrenaline 1 mg IV (10 ml of 1:10,000) and amiodarone 300 mg IV
- Continue giving adrenaline after alternate shocks ie fifth, seventh, ninth, eleventh etc
- If organised electrical activity is seen during a rhythm check, seek evidence of return of spontaneous circulation (ROSC)
- If present, commence post-resuscitation care
- Iif absent (PEA), resume CPR immediately and switch to the non-shockable algorithm
- If asystole is recognised during a rhythm check, switch to the non-shockable algorithm
Management of non-shockable rhythms (asystole or PEA)
- On recognising asystole, resume chest compressions immediately and continue for two minutes
- On recognising organised electrical activity, seek evidence of ROSC and if absent (PEA), resume chest compressions immediately and continue for two minutes
- After the first rhythm check, give adrenaline 1 mg IV (10 ml of 1:10,000)
- After two minutes, pause CPR to check the rhythm; on recognising asystole, resume chest compressions immediately and continue for two minutes; on recognising organised electrical activity, seek evidence of ROSC and if absent (PEA), resume chest compressions immediately and continue for two minutes
- After two minutes, pause CPR to check the rhythm; on recognising asystole, resume chest compressions immediately and continue for two minutes; on recognising organised electrical activity, seek evidence of ROSC and if absent (PEA), resume chest compressions immediately and continue for two minutes
- After the third rhythm check, given adrenaline 1 mg IV (10 ml of 1:10,000); continue giving adrenaline after alternate rhythm checks ie fifth, seventh, ninth, eleventh etc
- If a shockable rhythm is identified during a rhythm check, switch to the shockable algorithm but continue giving adrenaline after alternate rhythm checks: do not withhold until after the third shock
Factors to consider during CPR
- Ensure good quality CPR with minimal interruptions
- Establish and maintain a patent airway
- Consider airway adjuncts, supraglotic airway devices and definitive airways such as an endotracheal tube
- Once a definitive airway has been established, compressions and ventilations can be delivered continuously and simultaneously
- Establish intravenous (IV) access and take bloods including a venous blood gas (VBG)If IV access fails, use intraosseous (IO) access. You should switch to IO is access cannot be gained in under two minutes.
- If unable to obtain venous blood, do a femoral stab, which can be sent for all routine bloods and an arterial blood gas (ABG). An ABG should be obtained in either case as soon as possible.
- Recognise and treat reversible causes (4 H’s and 4 T’s)
- Hypoxia: ensure a patent airway and delivery of high flow oxygen
- Hypovolaemia: commence IV fluid resuscitation
- Hypo/hyperkalaemia and other metabolic derangements: check the VBG for any metabolic derangements and correct accordingly
- Hypothermia: check the patients temperature and if low re-warm to 32-34 degrees celcius
- Tension pneumothorax: auscultate the patient’s lung fields during ventilations and perform needle decompression as indicated
- Tamponade (cardiac): obtain a beside echocardiogram (echo) and perform pericardiocentesis as indicated
- Toxins: check the patient’s drug chart and/or enquire about recent medications in the collateral history
- Thrombosis: obtain a bedside ultrasound and identify symptoms and risk factors in the collateral history
Organise your team
- Delegate the tasks of airway management and ventilation, chest compressions, defibrillator operation, drug administration and time keeping to appropriate individuals; effective chest compressions are tiring so alternate individuals as necessary; as the team leader maintain an overview of the whole resuscitation attempt: stand at the foot of the bed, give clear instruction and do not get drawn in to performing individual tasks
Click here for medical student OSCE and PACES questions about Cardiac Arrest and Advanced Life Support (ALS)
Common advanced life support questions for medical students, finals, OSCEs and MRCP PACES
Click here to download free teaching notes on cardiac arrest and ALS: Cardiac Arrest
Perfect revision for medical students, finals, OSCEs and MRCP PACES
Advanced Life Support (ALS) Algorithm
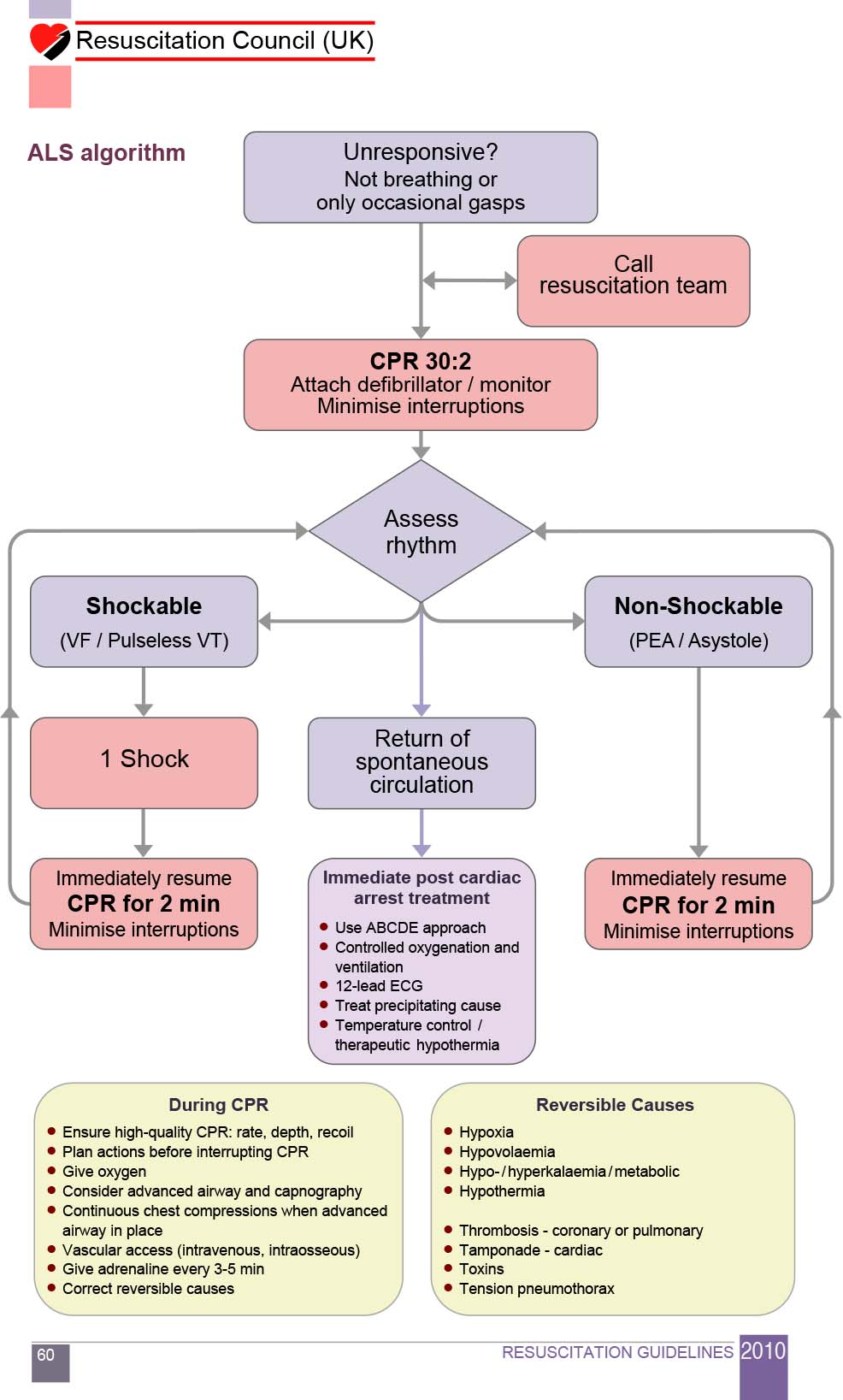
Advanced Life Support (ALS) Algorithm