


Heart blocks and bundle branch blocks on ECGs (EKGs)
In order to understand heart blocks it is important to have an understanding of the conduction system of the heart:
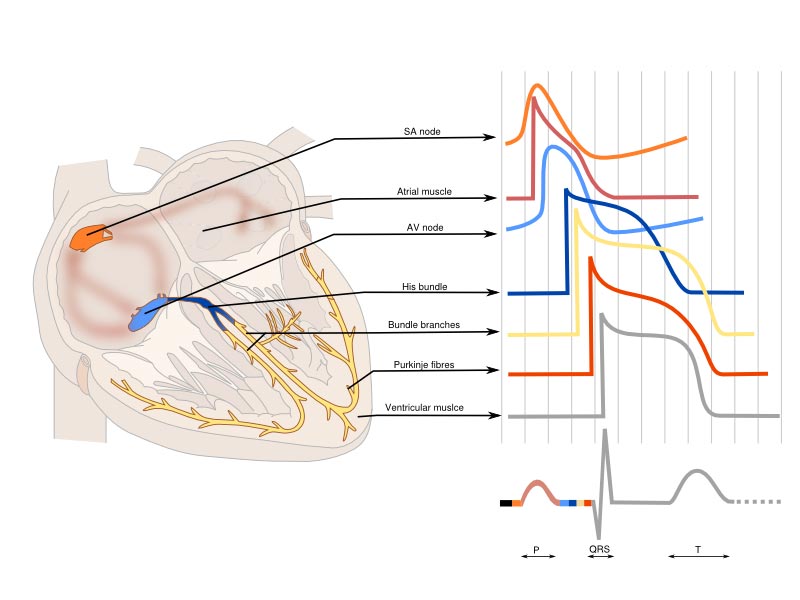
Passage of current through the heart
- The initial signal originates at the sinoatrial node (SAN)
- It is conducted through the myocardium of the atria and then passes via the atrio ventricular node (AVN) to the bundle of His. This bundle then splits into two bundle branches (left and right)
- The left bundle further splits into anterior and posterior fascicles (more on that later)
- Conduction continues through the Purkinjie fibres and finally into the ventricular muscle which contracts in systole which corresponds to the QRS complex
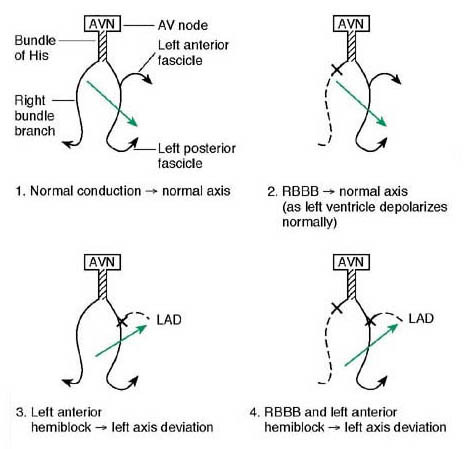
Below we discuss what happens when the conduction system is interrupted. The figure below gives an overview but we will look at each block in more detail.

1st degree heart block
1st degree block indicates slowed transmission of electrical activity through the AV node – therefore giving a prolonged PR interval. It can be a normal variant.

2nd degree heart block
There are two varieties of 2nd degree heart block to be aware of:
Mobitz type 1 (Wenckebach)
In Wenckebach block The PR interval prolongs from beat to beat and then one beat is not transmitted. This is a normal variant and requires no further investigation or treatment.
Mobitz Type 2
In Mobitz type 2 the PR interval is constant. However, there is an occasional non transmitted beat which may also be seen as 2:1 or 3:1 block – here there are alternate conducted and non-conducted beats.
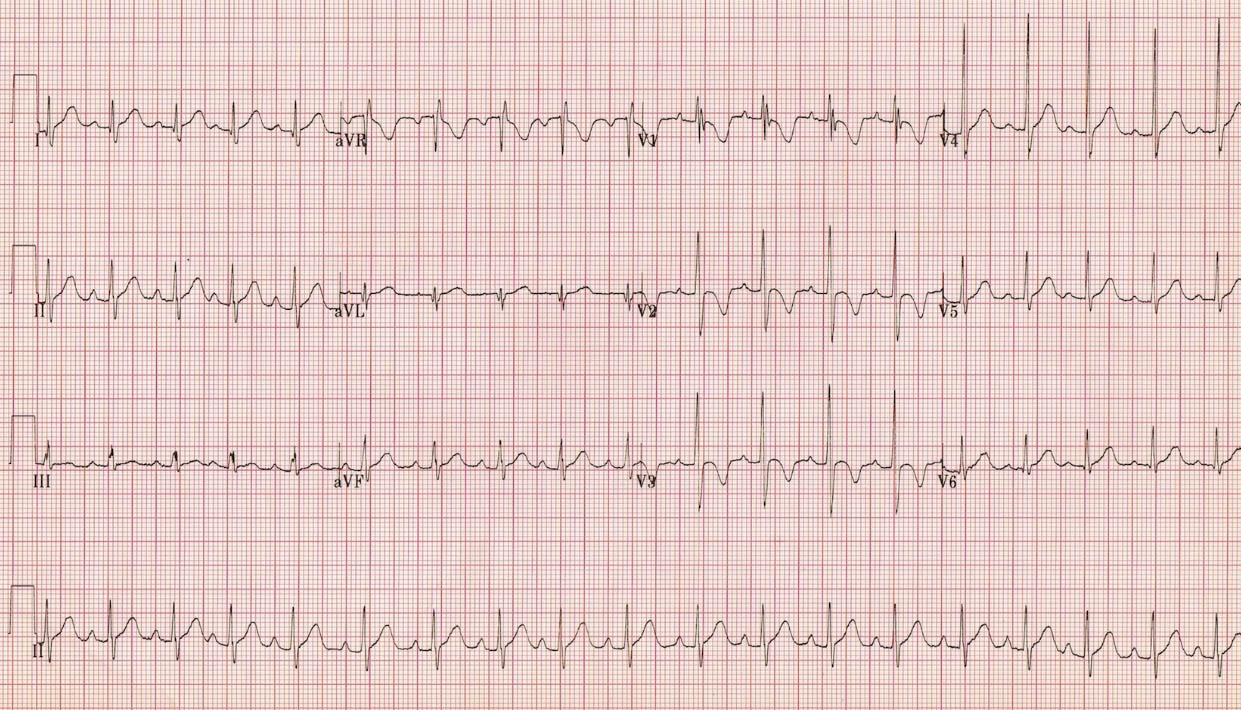
The above ECG shows 2:1 block with 2 P-waves for every one QRS
Significance of type 2 heart blocks
- Wencheback is a normal variant
- 2:1 and Mobitz type 2 blocks are pathological; they may precede 3rd degree or complete heart block
3rd degree heart block (complete heart block)
In 3rd degree heart blocks the connections between the atria and the ventricles are completely lost. The atrial rate continues as normal (as seen by regular p-waves). However, the actual heart rate is slow reflecting a ventricular escape rhythm which is generated from a focus within the ventricular muscle its self. Each p-wave is not associated with a QRS complex and the QRS complex is wide reflecting its ventricular origins.
Bundle branch blocks (BBBs)
Refer back to the figure below as you read about the different blocks:
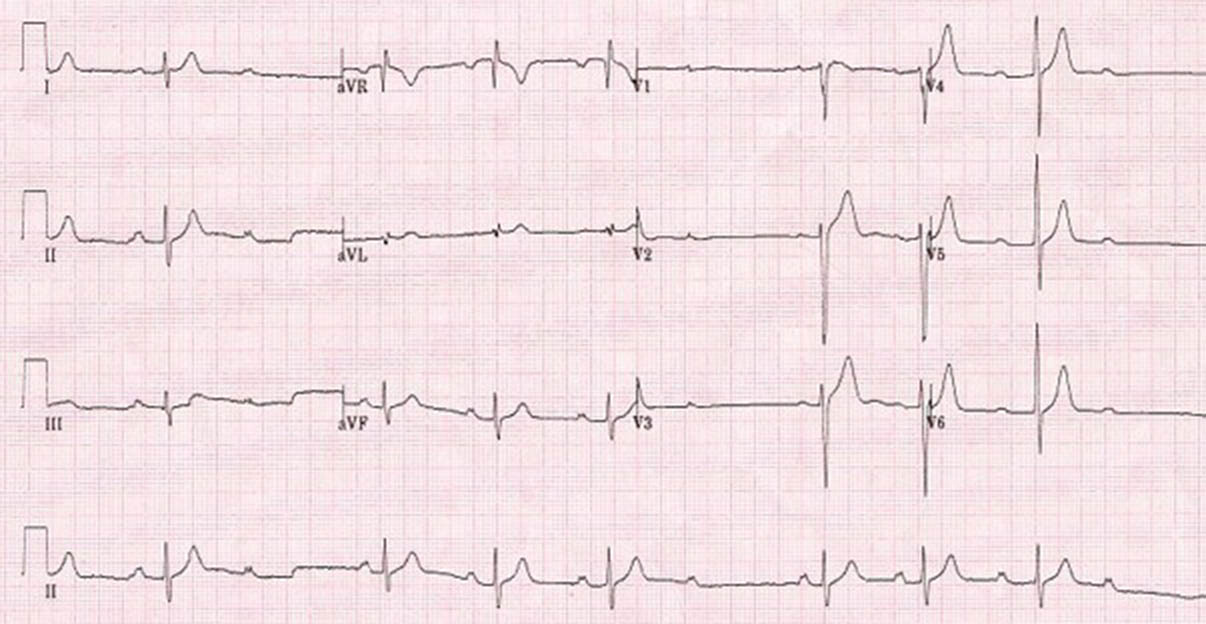
Right bundle branch block (RBBB)
- RBBB may be a normal variant – especially if the pattern is present but with a normal QRS duration.
- Otherwise it may indicate problems with the right side of the heart.
- In RBBB you will see wide complexes with a RSR pattern in V1 and deep S wave in V6.
How RBBB works
- From first principles RBBB occurs as left ventricular contraction happens just prior to right ventricular contraction (as the R bundle is not working) where they would normally contract together.
- Remember that the positive deflection is caused by depolarization travelling towards that lead. Therefore:
- Initially there is septal depolarization (left to right) causing a small R wave in V1 and Q wave in V6
- Then LV contraction causes an S wave in V1 and R wave in V6
- Then RV contraction causes an R wave in V1 and a deep S wave in V6
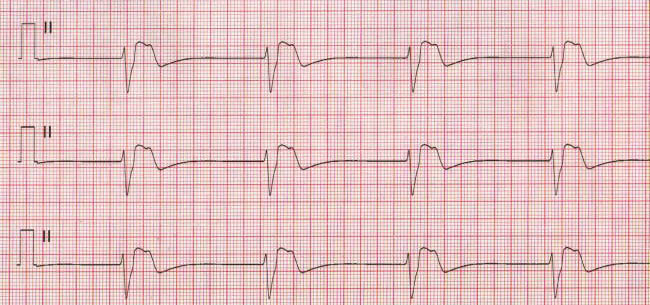
Left bundle branch block (LBBB)
This is always pathological and relates to left heart disease. If acute it may indicate acute myocardial infarction and is one of the indications for thrombolysis or transfer for PCI. This is one of the situations that illustrates the importance of having access to old ECGs.
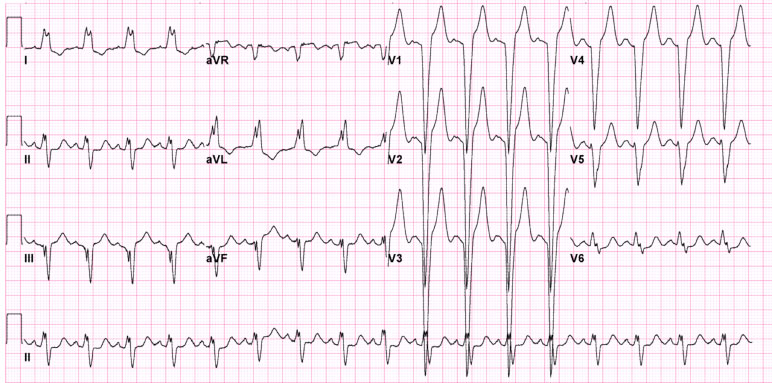
How LBBB works
- In LBBB you will see wide complexes with a negative (sometimes W shaped) complex in V1 and an M pattern in V4 -V6 and T wave inversion in the anterolateral leads.
- The T wave inversion is due to abnormal repolarization (after abnormal depolarization) rather than ischaemia.
- From first principles:
- The septum depolarizes from R to L causing a Q wave in V 1 and a R wave in V6
- The R ventricular contraction occurs first causing an R wave in V1 and a S wave in V6
- Then LV contraction causes an S wave in V1 and a further R wave in V6
Causes of bundle branch blocks (BBBs)
| Right bundle branch block (RBBB) | Left bundle branch block (LBBB) |
|
|
Fascicular blocks
- The left bundle can also be split into anterior and posterior fascicles (as shown in the figure above) and block can affect either of these.
- Anterior fascicular block
- If the anterior fascicle is blocked the cardiac axis swings round to the left causing left axis deviation.
- This is known as left anterior hemiblock
- It is often caused by LVH
- Posterior fascicular block
- Uncommonly the left posterior fascicle is exclusively blocked in which case there is right axis deviation.
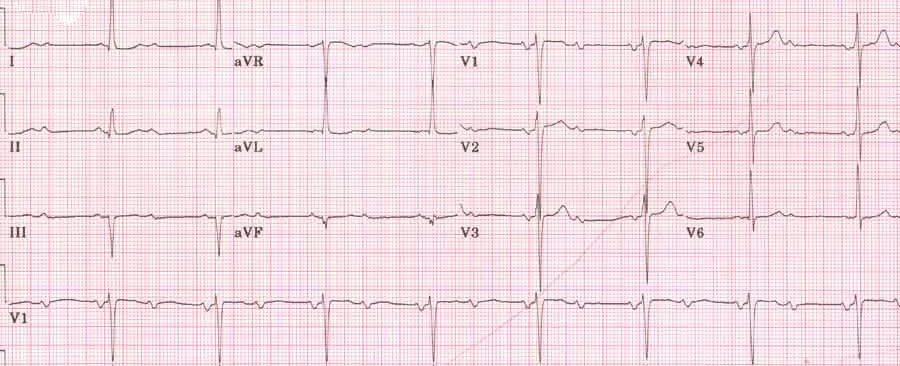
- Bifascicular block
- If the left anterior fascicle (or left posterior fascicle but this is much less common) and the right bundle are blocked you will see both right bundle branch block and left axis deviation, this is known as bifascicular block.
- This is clinically important as the patient may intermittently go into complete heart block as they are solely relying on the posterior fascicle for ventricular contraction.
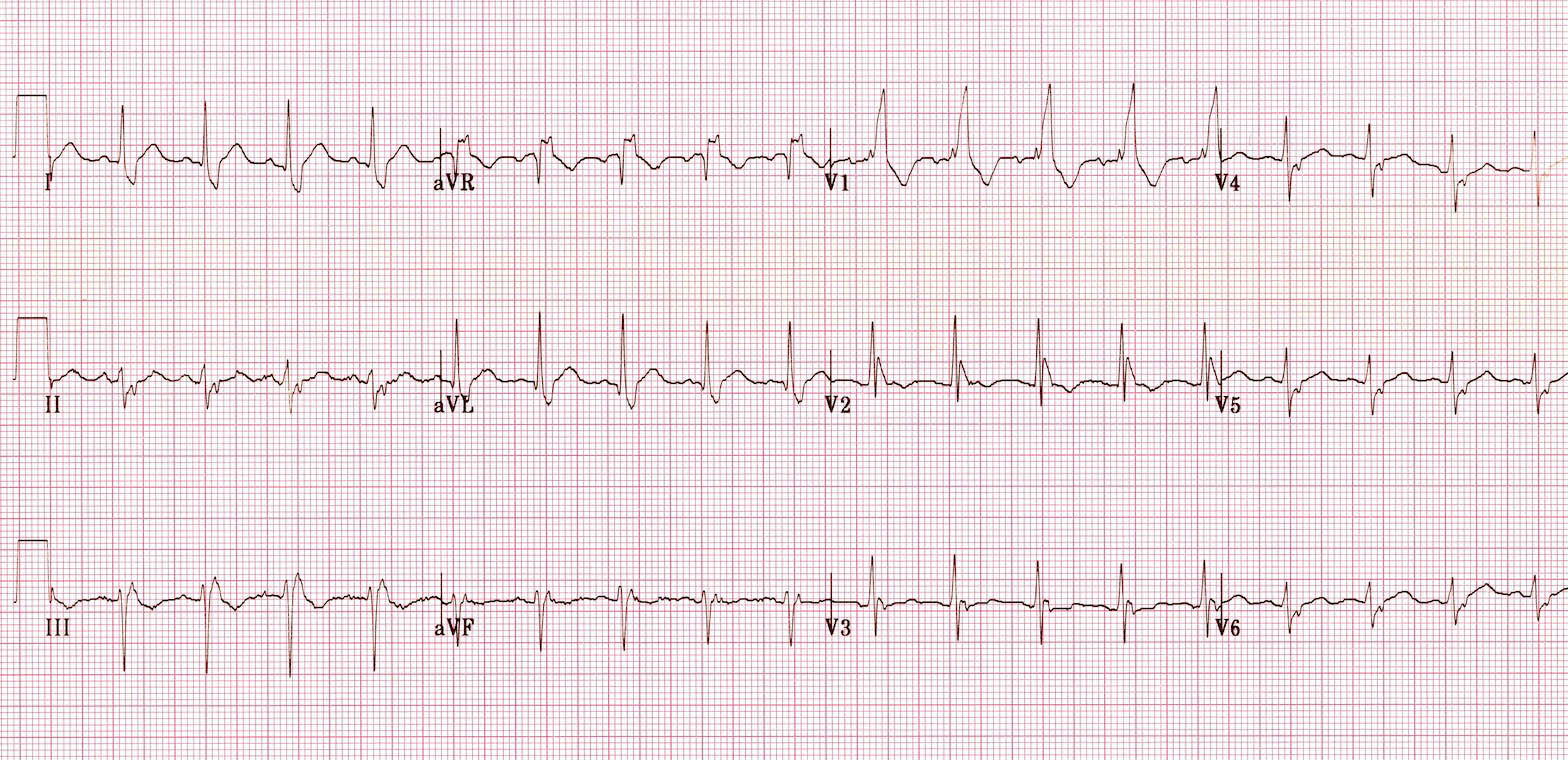
This ECG shows bifasicular block
Trifascicular block
- If there is bifasicular block with a prolonged pr interval (i.e. first degree block) this is known as trifasicular block as there is block in 2 fasicles and a delay in the 3rd
- As with bifasicular block it should be treated urgently as it may deteriorate into complete heart block
Click here for medical student OSCE and PACES exam questions about ECGs
Common ECG questions for medical students, finals, OSCEs and MRCP PACES
…and click here to read about the best way to interpret an ECG systematically